Please note: this article has been written in the plain English style, for laypeople who want to know more about D, but do not want scientific jargon, which only causes confusion. By necessity, some technical explanations are unavoidable. If you want anything explained further or have information worth adding to this, please do get in touch. In retrospect this also applies to the Vitamin C article recently added to this blog.
Vitamin D: Dangerous friend or generous foe?
Vitamin D is a vitamin that, in common with vitamin A, suffered the almost-universal reputation of being potentially dangerous if taken in more than just a token dose. Up until around 2,000 AD most doctors thought D levels took care of themselves and adding more than a small dose to our diets would be over-doing it. Once a cheap, easy test became available, it was discovered that deficiency of D is rampant and as research woke-up to this fact and got to work, many (but not yet all) realised that this vitamin had been seriously under-rated in it’s importance to human health.
What is vitamin D?
Actually vitamin D is more than one substance and more than just a vitamin. Foods we consume contain two types of D: D2 also known as Ergocalciferol comes from plant sources. D3 or Cholecalciferol (pronounced kolecalciferol) comes from animal sources (more about food later). Most of the research and recommendations to do with D are focused on D3 which is more potent and more useable than D2 (a recent study showed D3 is twice as effective as D2 at raising blood levels of D). A somewhat disconcerting meta-analysis of 90,000 people conducted a few years ago showed that people on D3 had a reduction in mortality (in other words did not die) of 6%. Good news but still disconcerting, because among people on D2 mortality went up by 2% – Bad news!You may ask what happened to D1? When it was first discovered D1 was indeed named, but it was then found that the substance was impure and was a mix of several chemicals including a pure form which was then isolated and renamed D2.
Vitamin D involvement in body chemistry.
Okay, so we will join the consensus in research and talk about D3 from here onwards.
D3 is a fat-soluble vitamin but it affects virtually everything inside our bodies because it is more than just a vitamin; it is in fact a steroid hormone! And hormones have major influence in our bodies. For example: Too much or too little thyroxin from our thyroid glands plays havoc with our bodyweight and energy levels. Failure of our pancreas to produce enough (or any) insulin renders us incapable of processing carbohydrate foods and without injections of insulin into the blood stream by our pancreas we would waste away and die even though we are still eating and drinking.
To understand the importance of D let’s have a simplified look at how it works inside our bodies. We all know that D is called ‘The sunshine vitamin’ because exposure of our skin to sunlight (or ultra-violet light) produces D inside us by converting 7-Dehydrocholesterol into D. Inactive D from our diet or from our skin is converted into its active form called calcitriol in our kidneys and is involved in bone-building. But that’s not all: Calcitriol is also manufactured in other body parts such as skin cells and immune cells. The difference here is the body’s use of calcitriol: These other sources of production are caused by inflammation and are connected to inflammatory diseases such as rheumatoid arthritis, multiple sclerosis, crohns disease etc.
Presently, scientists at the University of Wisconsin have created mice with kidney-specific D activation in order to observe the difference in the body, with the longer-term view hopefully yielding specific drugs that could target these diseases. There is a school of thought that thinks patients with mutations in their genome similar to the mice mutations, could be harmed by calcium supplementation such as we find being prescribed by doctors for bone health (and D is also not recommended if you have excessive blood levels of calcium, otherwise known as hypercalcaemia).

Vitamin D deficiency: A list of potential health problems.
There are not many foods that contain useful amounts of vitamin D3 but, until recent research started uncovering the huge potential D3 has, most doctors were inclined to say we get enough from being out in daylight. Now, informed opinion in the medical world states that it is probable that the vast majority of people in the Northern Hemisphere (well over half of planet Earths’ population!) suffer varying degrees of vitamin D deficiency and consequently more health problems in their lives. What happened to cause this? Our lifestyles have changed and whereas in the past (pre-industrial revolution) we lived in mainly rural economies and worked outside most of the time, now the majority of people work inside factories, offices etc, and therefore do not get enough sunlight. More recently, warnings about the sun causing skin cancer and premature ageing have persuaded many people to cover up and use sun block whenever they go out (in doing so their D production in their skin is completely shut off). The following points list various problems that can arise:
-
Extreme D deficiency during childhood can stunt growth and visibly distort the skeleton, the most well-known example of this being rickets: The mineralization of the skeleton is inadequate and the bones stay soft and legs bend outward as they cannot support the childs’ bodyweight and remember, this becomes a permanent disfigurement.
-
As an adult, D deficiency often leads to osteoporosis, a hollowing-out of the bones until they become very brittle. The most common cause of accidental death among the over-75s is breaking a hip as a result of a fall. The majority die within 6 weeks of their accident.
-
Osteomalacia: Again an adult problem, osteomalacia is softening of the bones due to loss of minerals. Known as ‘adult rickets’ this can twist you out of shape. Osteoporosis is
made worse by this and pain, especially in the joints, comes with it.
-
Heart disease/skeletal make-up: the heart is a muscular pump that never rests while we live. As with the rest of our muscles several minerals work together to keep it going, the principal players being calcium, magnesium, phosphorous, boron, and strontium. Pretty much all the vitamins we know are also involved, with D at the top of the list and vitamin K also important. We have been told to take in plenty of calcium for the sake of our bones, but without sufficient magnesium we are at risk of muscle cramps and nervous system agitation. Boron and strontium help maintain the architecture of our bones (no, it’s not the radioactive form of strontium!) and D and K also pitch in (note that boron, strontium and vitK are only needed in tiny amounts). Studies have shown low D levels can also lead to congestive heart failure.
-
Arterial problems: Calcium is present in bones and blood and as shown above it needs other substances to balance it; too much in the bones and we experience functional problems such as extreme cramps, too much in the blood and our arteries are in danger of ‘furring up’ over time until blood flow is reduced to a trickle and expiring from a heart attack becomes likely. What happens is, if any minor abrasions or cuts appear inside our arteries then calcium and cholesterol team up and create a patch that seals the leak. Too much calcium in the blood leads to bigger patches and too many patches eventually leads to an occlusion (blockage) which could be fatal. Ironically, too much bone-building material i.e. calcium in our blood puts us at risk in this way and still cannot protect our bones.
-
High blood pressure: As arteries and capillaries become narrower so blood pressure inevitably goes up.
-
Problems with pregnancy: Newborns that have an exceptionally sweaty face and head usually have very low D levels. Research into fertility problems implicates low D levels with polycystic ovary syndrome (PCOS), a major cause of female infertility. Even as an adult, if you experience sweaty forehead for no apparent reason, it is almost certainly caused by low D levels.
-
In parts of the world with significantly less sunlight for several months out of the year (for example Finland, Alaska, Siberia), depression due to lack of sun exposure is common and in many of these places is treated as a very serious medical issue. Inhabitants are encouraged to purchase light boxes, devices that emit therapeutic light that will help them maintain vitamin D levels during dark winter months.
-
Chronic infections and illnesses: D is known to effect over 2,700 genes in our bodies and our immune system is tied in with these DNA strands. Low levels of D leave us more vulnerable to many diseases, including viral infections and there does seem to be a connection between chronic diseases such as diabetes and low levels of D.
-
Respiratory difficulties: Finding it hard to breathe sometimes? Or perhaps you have asthma? As D deficiency has increased over the years the number of young people with asthma has also multiplied. Years ago when I was in primary school there was only one child I knew of that had asthma. Now if I were to visit that same school there are up to a third of the children in each classroom with asthma.
-
Fatigue: Feeling bone-weary (literally!) is a well-known effect of low D levels. Pain deep within the joints and bones usually accompanies this lack of energy. Athletes that inexplicably begin to lose stamina during training have recovered by upping D intake to match their strenuous lifestyles.
Cancer: A lot of studies have examined the effects of higher or lower levels of D on various cancers and briefly summing it up there is a positive correlation between higher D levels and more favourable outcomes for cancer patients.
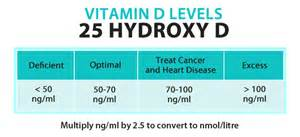
Okay my friends, the list above is not comprehensive, there are many more problems caused by low D levels but looking at the problems listed it’s more than enough for me! This is one occasion when it would appear that complicated remedies are not required, supposedly all we have to do is get more sunshine and/or take a D supplement and get our blood levels up to 40ng/ml (nanograms per millilitre) or higher (up to 100ng/ml is considered to be acceptable by some researchers but the majority think 50 to 70ng/ml is an optimal range). Ask your doctor for a blood level test of vitamin D: The test is called 25(OH)D or 25-hydroxyvitamin D. Test in the month where levels will naturally be highest (August) and lowest (February). If you live ‘down under’ you take the same test but it reads back to front because of the opposite seasons. If you only test once a year make it at the end of Winter when your levels will be at their lowest.
Things that affect absorption of D and answers to these problems.
Notice I said ‘supposedly all we have to do’ above. In fact, it is not that easy. Several things influence D absorption – and if you don’t absorb it it’s as if you never took it.
-
Dark skin. African and Asian people have darker skin because they are adapted to living in hot, sunny climates for most if not all of the year. Moving to cooler countries with dark cold winters’ such as most European countries experience means they will inevitably run low on D as the winter produces nothing in their skin, and even our summers most of the time are not as sunny as they need. The only answer is supplements as their traditional diets lack D, the intense sun in their countries of origin being enough for them to stay healthy without needing food sources of D.

-
Age. We all know that everything seems to work less efficiently in our bodies as we age and sure enough a person at 70 years old will produce over 30 percent less D when out in the sun compared to when they were 30 years old. More sun exposure may help but it may be too much for our older skin to cope with long-term. The safest alternative is supplements again.
-
Gut problems such as crohn’s disease, Inflammatory Bowel Syndrome (IBS) and gluten intolerance make it more difficult to absorb D from food so once again supplements can help. This is not an endorsement but merely what I take myself: I use a liquid vitamin D3/K2 supplement which can be put on cereal or dinner or any food so long as the food contains some fat to help it to be absorbed. At a cost of around £20.00 for a little bottle it may sound expensive but you get 600 doses so it works out to 3.3 pence per day and includes vitamin K2 which is the preferred form of K to balance D intake.
-
Renal (kidney) disease. If you have made it this far reading this article you will recall that D is activated and becomes calcitriol in our bodies as a result of processing through our kidneys. Kidney failure leading to dialysis severely reduces the capacity of the kidneys to do this. To find out if your kidneys are in good health ask your doctor for a test to assess your eGFR (estimated glomerular filtration rate). If it is below 60 ml/min, you would fall in the stage 3 (or higher) category of chronic kidney disease (called CKD 3 which is very common in older people, especially if they suffer with high blood pressure and/or diabetes, and also take medication that may affect kidney function). It’s something to discuss with your GP, including your vitamin D levels, and whether supplementing your diet with D3 would be a good idea for you.
-
Obesity: Because it is fat-soluble extra fat on our bodies acts as a ‘fat sink’ absorbing D and tending to hang onto it. Potentially even a good intake of D may not be enough if we become very fat, in which case taking a bigger dose of supplements may be necessary. Don’t think if your extra weight is composed of muscle (i.e. you are a bodybuilder or a rugby player or other type of large muscular athlete) that this does not apply to you because it does! Whether your extra bulk is fat or muscle the mere fact that you are larger means your body needs more D than Mr or Mrs average!
-
Prescription medicines: Taking a mix of different medicines each day puts us into the unknown zone as far as side-effects go, yet many of us (particularly the seniors) are in that situation. Anti-epilepsy drugs are known to interfere with D absorption and steroid drugs such as are found in asthma inhalers are also a problem. Because different people are on different types of medicines there are probably many more drug interactions going on that we know nothing about.

Food sources of D
As a fat-soluble substance the best sources of D include fats and stating the obvious fat-free sources such as some supplements should be taken with food or drink that contains fat. The following list is nowhere near comprehensive but it may give some ideas on what to eat.
Salmon is a very good source of omega-3 fatty acids and as an oily fish the D3 content is spread throughout it’s whole body. Generally 3 ounces (85grams) of red salmon contains 800iu of D3 versus 370iu in pink salmon.
Halibut (3 ounces = 200iu of D3) and trout (3 ounces = 650iu) are white fish. Unlike salmon or mackerel or sardines they concentrate oil and vitamins in their livers (cod liver oil for example) but white or oily, fish is a good addition to our diets.
Some D -free foods are fortified with vitamin mixes that include D3, which then can contribute to our total D intake. The most popular of these foods are breakfast cereals and milk alternatives like soya milk, almond milk and rice milk which are also fortified with calcium as well as D. ‘Real’ or dairy milk is fortified in the USA but not in the UK.
Eggs contain around 40iu of D3 if you eat the whole egg (no, not including the shell!) as the D content is found in the yolk along with the eggs’ fat content. Many bodybuilders diet for contests by cooking with egg whites only, throwing the yolks away to avoid the fat content. By doing so they are missing out on the lecithin, fat, vitamin A and D and sulphur-based amino acids content which make eggs a good food source.
Mushrooms: Chanterelle, portabello and maitake mushrooms contain significant amounts of D (bear in mind this will be D2 not D3) and maitake in particular can help to lower blood pressure and reduce the risk of getting diabetes. As an interesting aside, when these mushrooms are grown under ultra-violet light they are even more nutritious than in the wild.

Supplemental vitamin D.
Unlike vitamin C with it’s plethora of types of C vitamin, D is much more straightforward. Pretty much any supplemental D from powders to tablets or capsules or liquids have the same effect and most of the D3 out there is quite cheap. Remember to count the D from your diet and from your multi-vitamin as well as your specific D supplement – how we can allow for sunshine is anyone’s guess! As I said earlier I take a liquid mix of D3 and K2 (sounds like a mountain range!). 2 Drops contain 1,000iu of D3 and 200 ug of K2 and costs 3.3 pence. That’s right, it can be that cheap and is still good quality!
Vitamin D overdose: What are the chances of it happening?
The SUL (Safe Upper Limit) for vitamin D in the UK is currently set at 2,000iu (international units) per day. Contrast that with the USA where the SUL stands at 4,000iu. By the way, D amounts can be listed in ug (micrograms) as well as iu’s. To convert, divide iu amount by 40 (for example, 2,000iu equals 50 ug).
Most of the medical evidence relating to D suggests much higher amounts can be tolerated and many doctors are now of the opinion that 2,000iu is nowhere near the real safe limit. The UK Recommended Daily Intake (RDA) is 600iu, a pathetically low figure. Experiments on people with multiple sclerosis and people with colds and flu show insignificant benefits are derived from such low doses. Type-1 diabetes also shows some response to higher doses, the chances of contracting the illness reducing with greater intakes. Low blood levels of D are often found in people with Parkinson’s and this goes hand-in-hand with the fatigue commonly experienced by many Parky people. Supplements are necessary to raise blood levels: I have personal experience of this when (don’t try this unless you are under a doctor’s supervision and monitoring as I was) I took 100,000iu of D3 per day for a whole month! This raised my blood level of D3 from sub-30 to 91 and I maintain at around 70 by taking 2,000 to 4,000iu per day. Like me, many Parky people seem to generate very little D from sun exposure and low amounts in food are not enough. Again, supplements are the answer.
For the sceptics among you: If you think that was a huge dose to take, read this! It is a common practice worldwide for doctors to treat infants suffering with rickets by giving them a one-off D3 injection (this is known as ‘Stosstherapy’) of 600,000iu!!
One researcher talked about how some doctors still have a fear of recommending more D3 to people with low levels, thinking that the chances of overdosing from taking larger amounts of D3 are much greater than they really are. He said it was like dying of thirst in the middle of a desert yet being afraid of taking a sip of water if any could be found.
I personally feel that there is more than enough evidence noted above to convince me that it is a fact that many of us need more D – but please, take the blood tests or else you would just be running blind as to how much you need to reach an optimal intake for your health.
LMMC

First of all may I say how impressed I am with this article – Lionel has produced a thoroughly informative description of a complex subject in a style and manner that the lay person can relate to and understand.
My interest in Vitamin D3 goes back to diagnosis when a routine blood test identified a surprising deficiency, despite it being summer and me spending several daily hours outdoors – I should have been awash with D3, yet there I was, languishing at the foot of the chart! Yet another example of Parkinson’s unexpected interference with your metabolism!
Fortunately, as Lionel explains, there is a solution readily available in the way of supplements. I now take these daily and monitor levels every nine months or so before my movement disorder specialist’s appointment. Into its fifth year, my ‘D3 deficiency chart’ provides some interesting viewing.
If you haven’t done so already consider following Lionel’s advice and book that appointment – after all, once you’ve digested Lionel’s article and realised how wide reaching the effects of this steroid hormone cum vitamin really extend, you’ll never be able to look at D3 in the same way again!
roger9@prestoncapes.org .uk
>
LikeLike